What is a Rotator Cuff Tear?
- benwilliams801
- Jun 4
- 9 min read


A rotator cuff tear doesn't have to mean months of open surgery and a difficult recovery. For many patients, arthroscopic repair offers a path back to full function with less pain, smaller incisions, and a faster return to daily life.
The rotator cuff is a group of four muscles and their tendons that wrap around the shoulder joint, keeping the ball of the upper arm bone seated securely in the socket. When one or more of these tendons tear — whether from a sudden injury or years of gradual wear — the shoulder can lose significant strength and range of motion.
In my practice, I approach every rotator cuff tear individually. Not every tear requires surgery — many partial tears respond well to physical therapy and targeted treatment. But for full-thickness tears, or for partial tears that haven't improved with conservative care, arthroscopic repair is often the right next step.
What is arthroscopic repair?
Arthroscopy is a surgical technique that uses a small camera — about the width of a pencil — inserted through a tiny incision. The camera transmits live images to a monitor, allowing me to see inside the shoulder joint with clarity that would be impossible through a small open incision. Additional small portals are made to introduce the instruments needed to repair the tendon.
Rather than opening the shoulder through a large incision, the entire repair is performed through these portals. Anchors — small implants made of bioabsorbable material — are placed into the bone, and strong sutures are passed through and around the torn tendon to secure it back to where it belongs.
How the procedure works
Assessment
— Once inside the joint, I carefully evaluate the full extent of the tear, the quality of the tendon tissue, and the condition of surrounding structures including the biceps tendon and joint lining.
Preparation
— The torn tendon edge is debrided and the area of the bone where it will be reattached is prepared to create a healthy surface that promotes healing.
Anchor placement
— Small anchors loaded with sutures are placed into the bone at the site of reattachment.
Tendon repair
— Sutures are passed through the tendon in a pattern designed to distribute force evenly and maximize contact between the tendon and bone.
Closure
— The portals are closed with a single suture or adhesive strips. A sling is applied, and you go home.
Who is a good candidate?
Arthroscopic repair works well for a wide range of patients, but the best outcomes tend to occur when certain factors are in place. We discuss all of these at your consultation:
Full-thickness tear confirmed on MRI
Partial tear that has failed 3–6 months of physical therapy
Tendon tissue that is healthy enough to hold repair (retraction and atrophy matter)
Reasonable overall health and no active infection
Patient commitment to the post-operative rehabilitation process
Older, massively retracted, or severely fatty-infiltrated tendons may not be suitable for repair. In those cases, we discuss alternative procedures — including tendon transfers or reverse shoulder replacement — that can still restore meaningful function.
A note on timing
Acute tears in younger, active patients are often best repaired promptly — within weeks to a few months of injury — before the tendon retracts and the muscle begins to atrophy. If you've had a sudden injury and are experiencing significant weakness, it's worth getting an MRI and a surgical opinion sooner rather than later.
Recovery and rehabilitation
I tell every patient the same thing: the surgery takes an hour or two, but the healing takes months. That isn't a discouragement — it's a reflection of biology. Tendon-to-bone healing is a slow, gradual process, and the rehabilitation program is designed to protect that healing while steadily restoring movement and strength.
Weeks 1–6
— Sling protection. Passive range-of-motion exercises guided by a physical therapist begin within a few days. The goal is to keep the shoulder moving gently while the tendon heals to bone.
Weeks 6–12
— Active-assisted and then active motion. The sling comes off and you begin working the shoulder with your own muscle power, initially with support.
Months 3–6
— Progressive strengthening. Resistance exercises are introduced gradually as the repair matures and the tendon grows stronger.
Months 6–12
— Return to full activity, including sport and manual labor, for most patients. Overhead athletes may require up to 12 months before returning to throwing.
Most patients notice meaningful improvement in pain within the first few weeks, even while range of motion is still limited. Full strength recovery takes longer — typically 6 to 12 months — and that timeline is worth understanding before surgery so expectations are grounded in reality.
Risks and realistic expectations
Arthroscopic rotator cuff repair is a safe procedure with a well-established track record, but no surgery is without risk. The risks we discuss most often include:
Re-tear of the repaired tendon (most common in large or massive tears)
Stiffness or limited range of motion
Infection (rare with arthroscopic technique)
Nerve or blood vessel injury (uncommon)
Anesthesia-related complications
Overall, clinical studies consistently show high patient satisfaction and meaningful functional improvement following arthroscopic repair — particularly in patients with smaller to medium-sized tears who commit to the rehabilitation process.
If you have questions about your shoulder or whether this procedure might be right for you, I'm glad to talk through the specifics at a consultation. Every shoulder is different, and getting the right diagnosis is always the first step.
Ben Williams, MD
Comprehensive Orthopedics and Sports Medicine
801-533-2002
Arthroscopic Rotator Cuff Repair
What to expect before surgery
Dr. Williams and/or Sean Kendall, PA-C will go over the results of your imaging and go over the risks of surgery and pick a date
We will obtain authorization from your insurance for the surgery
The hospital will call the afternoon before with instructions for the day of surgery such as when to stop eating and drinking, what medications to stop, and when to arrive.
All GLP-1 agonists (Ozempic, Wegovy, Mounjaro, etc.) will need to be stopped at least a week before surgery). Most blood thinners need to be stopped 5 days before surgery.
What to expect the day of surgery
The anesthesiologist will discuss a nerve block
The surgery will take approximately 1-2 hours
You will wake up with a sling and an ice machine. The nurses will show you how to get dressed and how the sling and ice machine work before you leave.
What to expect the first few days after surgery
You will be prescribed narcotic pain medication. If you get a nerve block, your arm will likely be numb for around 20 hours. Take 600-800mg of ibuprofen (unless you cannot take NSAIDs) on the evening after surgery. Take this every 8 hours for the first few days and supplement with the narcotic pain medication as needed.
Remove sling only to change your clothes. Wear your sling at all times, including while sleeping, for 6 weeks.
Use the ice machine as long as needed.
Keep your incisions dry. You can cover up the dressing with Glad Press-n-Seal in order to shower.
Call and make an appointment for 10-14 days after surgery to remove your sutures.
Rotator Cuff Repair: Patient Recovery Guide
This handout outlines what to expect following your rotator cuff repair surgery and the different phases of recovery. Please follow your surgeon's specific instructions, as individual recovery may vary.
Phase 1: Protection and Passive Motion (0-6 weeks)
Wear your sling at all times, including while sleeping, for 6 weeks
Remove sling only for showering and prescribed exercises
Focus on pain reduction and tissue healing
Perform passive range of motion exercises as directed by your surgeon
Avoid active shoulder movements or reaching behind your back
Phase 2: Active Motion (6-12 weeks)
Your sling will be removed at the start of this phase
Begin formal physical therapy 2-3 times per week
Gradually return to active movements and functional range of motion exercises
Continue to avoid motions behind your back for 8 weeks post-surgery
Phase 3: Strengthening (12-22 weeks)
Focus on strengthening exercises for the rotator cuff muscles
Use light resistance bands or weights as directed by your therapist
Continue stretching exercises to maintain and improve range of motion
Phase 4: Full Activity (4-6 months and beyond)
Gradual return to full activities and sports, as approved by your surgeon
Continue home exercise program to maintain strength and flexibility
Full recovery may take 4-6 months, with maximum improvement up to 9-12 months
Important Reminders:
Follow your surgeon's and physical therapist's instructions carefully
Attend all scheduled follow-up appointments and therapy sessions
Be patient with your recovery; healing takes time
Contact your healthcare provider if you experience increased pain, fever, or other concerning symptoms
Remember, everyone's recovery is unique. Your healthcare team will guide you through each phase based on your individual progress and needs.
Background:
What is an Arthroscopic Rotator Cuff Repair?
The principle of arthroscopic rotator cuff surgery is to reattach the torn tendon back to the humerus (ball) and address any other areas of concern at the same time – biceps tendon, shoulder spur, bursitis, acromioclavicular joint, and shoulder joint capsule. The procedure is almost always carried arthroscopically and is an outpatient surgery. Patients are in a sling for six weeks and start physical therapy at four weeks post-surgery.
What conditions does an Arthroscopic Rotator Cuff Repair treat?
The main area of concern is the torn rotator cuff (supraspinatus tendon tear is the most common); the following areas are also addressed if needed:
Biceps tendonitis
Acromioclavicular joint (AC Joint) arthritis
Subacromial bursitis
Subacromial spur (Shoulder spur)
Shoulder joint capsulitis
Glenoid labrum tear (anterior and/or posterior labrum)
The decision to address these areas is best made in the office during your consultation – this is based on a careful history, physical examination, imaging review (MRI), and discussion with the patient about their expectations and functional requirements. In a small number of cases, unexpected findings are made at surgery and Dr Williams will undertake the treatment that provides you with the best outcome.
How is an Arthroscopic Rotator Cuff Repair performed?
The procedure is performed under a General Anesthetic
Small key-hole incisions (about ½ inch long) are made and the camera and surgical instruments are placed inside the shoulder. Usually 4-6 incisions are enough to carefully repair the shoulder
A thorough 15-point examination of the shoulder joint is made via the arthroscopic camera and pictures are taken to document findings.
Biceps
The first step is to address the biceps tendon if needed
The biceps tendon will either be moved out of the shoulder joint or re-anchored in the armpit at the start of the case. Studies have shown that in most cases, simply detaching the biceps tendon will not affect function and will relieve biceps-related pain.
Bone Spur and Bursa
Next, attention is turned to the area above the tendon and any bursitis is shaved away carefully and the bone spur is identified.
A special 5.5mm metallic burr is then used to shave away the spur and create more room to allow the tendon to move freely.
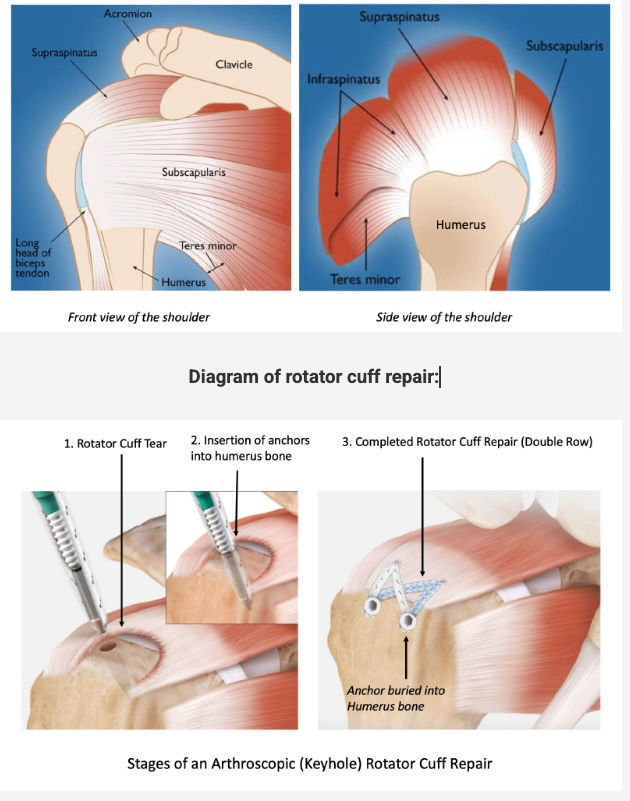
Rotator Cuff Tear
If there is a tear (as identified on the MRI pre-surgery) then it is carefully assessed and cleaned up. The tear is mobilized to allow for a tension-free repair and the Humerus (ball) is prepared to accept the anchor.
Suture anchors are then placed into the Humerus (ball of the shoulder joint) and sutures are passed through the tendon and repaired to bone (as seen in the picture below)
There are many special techniques to obtain a good repair and your shoulder surgeon is well versed in this.
AC Joint Resection
If this joint was identified as a pain generator during your examination, then about 7mm of bone from the end of the collar bone is removed.
All of the wounds are then closed and dressings applied. Your arm will be placed in a sling.
Diagram of rotator cuff repair:
Click this link if you would like to watch an animation of one of the most common repair techniques used by Dr. Williams:
What are the risks of Arthroscopic Rotator Cuff Repair?
General Shoulder Surgery Risks
Surgery is a carefully choreographed process and you are being treated by a sub-specialist shoulder surgeon and a highly experienced team; however, all surgeries inherently carry some risk of complications, such as (all are below 1%). General risks include:
Infection
Nerve injury
Bleeding
Failure of the repair to heal
Specific Shoulder Surgery Risks
Frozen Shoulder
Frozen shoulder occurs when the shoulder joint capsule becomes inflamed, red and scarred – it initially presents with severe pain, then progresses to stiffness and thaws out over many months
After routine shoulder surgery, the risk of frozen shoulder is 5%
There is nothing your surgeon can do to reduce this risk
This risk is around 10% if you have a history of Diabetes or Thyroid disorders.
Occasionally the frozen shoulder will not improve with physical therapy and another operation may be necessary
Reoperation and failure of surgery
When performing a shoulder reconstruction, your surgeon is using your own tissue to repair what is damaged. The weakest point in the repair is your own tissue. The longer the history of damage and frequency of trauma prior to surgery, the more likely the tissue quality is poor. Other factors like Smoking and Diabetes may also reduce your tissue quality. The risk of re-tear or non-healing of the tendon is around 5-20%, but can be much higher in older patients with very large tears.
Driving after shoulder surgery
It is not advisable to drive while you are wearing the sling (first 6 weeks). However, some patients do drive a limited amount after they are off of the narcotic pain medication.
Showering and getting dressed
You may take the sling off to shower
Lean forward and allow your arm to “dangle” to wash under your arms
Keep the dressings dry for the first 4 days.
When getting dressed, you may use your good arm to move your affected (operated arm) to place your arms through the sleeves carefully
Sleeping after Shoulder Surgery
Most patients find it difficult to lie flat after shoulder surgery.
Consider using a recliner or few pillows to prop yourself up and sleep at a slight incline; this may be necessary for 4-6 weeks after surgery. You should keep your sling on while asleep.
Elbow and hand movement
Keep your elbow and hands joints moving and supple for the duration of time you are in the sling. The best time to move your elbow (into full extension and flexion) is when you are in the shower, just out of the shower and about to get dressed.
Video on how to sleep after shoulder surgery:
How to get dressed and undressed after shoulder surgery:



Comments